
Just Do the 12-Lead: How Sneaky Cardiac Calls Can Fool You
There’s a moment that lives rent-free in my brain: a patient, mid-60s, pale and diaphoretic, insisting their only complaint is “a little indigestion.” No chest pain, no radiation, nothing textbook. My gut said something was off, so I slapped on a 12-lead.
STEMI. Right there, plain as day.
That moment taught me a lesson I’ll never forget: when in doubt, just do the 12-lead.
Cardiac Doesn’t Always Look Cardiac
We train for the “classic” presentation—substernal chest pain, radiating to the left arm, nausea, diaphoresis. And yes, sometimes it really is that clean.
But often, it isn’t.
Cardiac problems can show up as:
Epigastric discomfort
Fatigue or generalized weakness
Shortness of breath without chest pain
Syncope or near-syncope
Jaw, neck, or back pain
Nausea or unexplained anxiety
And yes—sometimes even just a gut feeling that something isn’t right.
Who’s Most Likely to Fool You?
1. Elderly Patients
Their pain responses are often blunted, and they may not experience or express classic symptoms.
“I just feel off” might be their version of a full-blown MI.
2. Diabetics
Neuropathy can mask pain, and they may only present with weakness, dizziness, or vomiting.
3. Women
Studies continue to show that women are more likely to have atypical cardiac symptoms—and more likely to be misdiagnosed.
The 12-Lead Is Fast, Cheap, and Tells the Truth
It takes less than 2 minutes. It costs nothing. It could change everything.
I’d rather run a dozen normal 12-leads than miss the one that matters. That strip could be the difference between a code in the driveway and a cath lab save.
So why do we hesitate?
Sometimes it’s pressure to move quickly. Sometimes it’s a partner or provider who minimizes the symptoms. Sometimes it’s just habit—we don’t expect the cardiac issue because the story doesn’t sound like one.
But the heart doesn’t care what we expect. It’ll sneak up on us anyway.
Real Talk from the Field
I’ve seen cardiac events hide behind vague complaints more times than I can count. The ones that still haunt me aren’t the screaming chest pains—they’re the “I almost didn’t call you” patients who looked stable but were crashing inside.
And yeah—every time I’ve trusted my gut and run the 12-lead “just in case”, I’ve never regretted it.
Pro Tips: Make the 12-Lead Your Reflex
Any chest pain = 12-lead
Any unexplained SOB or syncope = 12-lead
Any “something’s not right” feeling = 12-lead
Any patient over 50 with vague complaints = 12-lead
Any diabetic, elderly, or female patient with odd symptoms = 12-lead
Even better? Run serials. Get one early, and repeat en route if the story evolves. Subtle ST changes over time can be a game changer.
Final Thought: It’s Just Stickers and a Strip—But It Can Save a Life
Cardiac calls are sneaky. Don’t let a clean story fool you. The patient isn’t lying—but their heart might be.
So next time you hesitate, hear this in your head:
Just do the 12-lead.
STEMI recognition is time-sensitive — and cognitive overload doesn’t help.
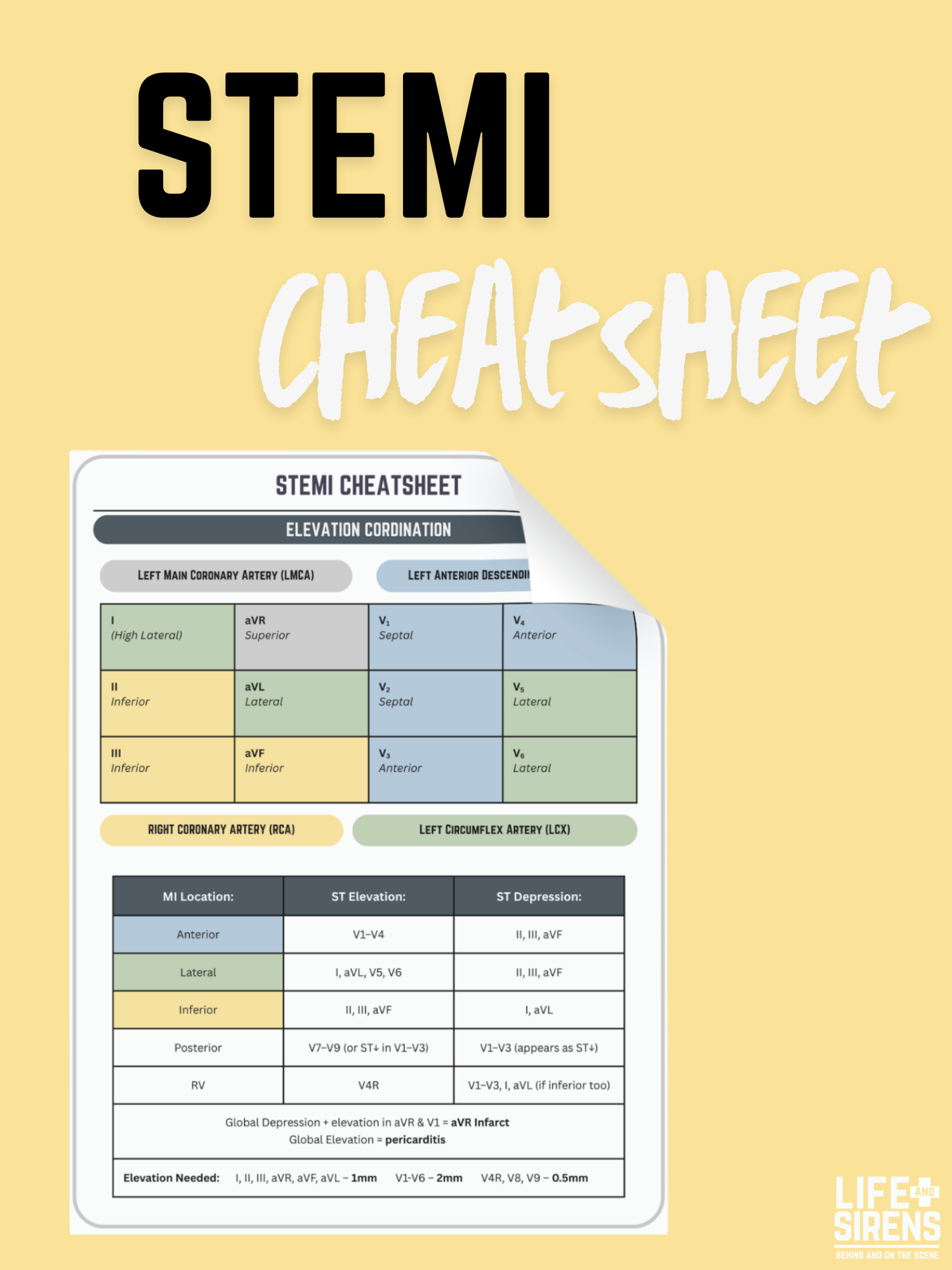
The Life & Sirens STEMI Cheatsheet is a focused, one-page reference designed to support rapid ECG interpretation and infarct localization during high-acuity cardiac calls. This resource organizes ST-elevation patterns by lead group, correlates them with myocardial regions and coronary arteries, and highlights key reciprocal changes that matter in the field.
Built for EMS providers, this cheatsheet is ideal for quick review, education, and reinforcement when seconds count and clarity matters.
What This Cheatsheet Covers
ST-elevation patterns by lead group
Infarct location identification (anterior, inferior, lateral, posterior, RV)
Corresponding coronary arteries (RCA, LAD, LCX, LMCA)
Expected reciprocal ST-segment changes
Posterior and right-sided MI recognition
Special patterns (global elevation vs depression, aVR considerations)
ST-elevation measurement thresholds by lead location
Why This Resource Works
Clear visual organization for fast pattern recognition
Reinforces STEMI localization without overcomplication
Supports confident activation and communication
Useful for training, refresher review, and simulations
Designed from a prehospital perspective
Product Details
📄 Format: Digital PDF download
🖨 Print Size: Full page
⚠️ Disclaimer
This resource is provided for educational and informational purposes only and does not replace clinical judgment, medical direction, local protocols, or formal training. Always follow your agency’s guidelines and medical oversight.